Updated July 27, 2023
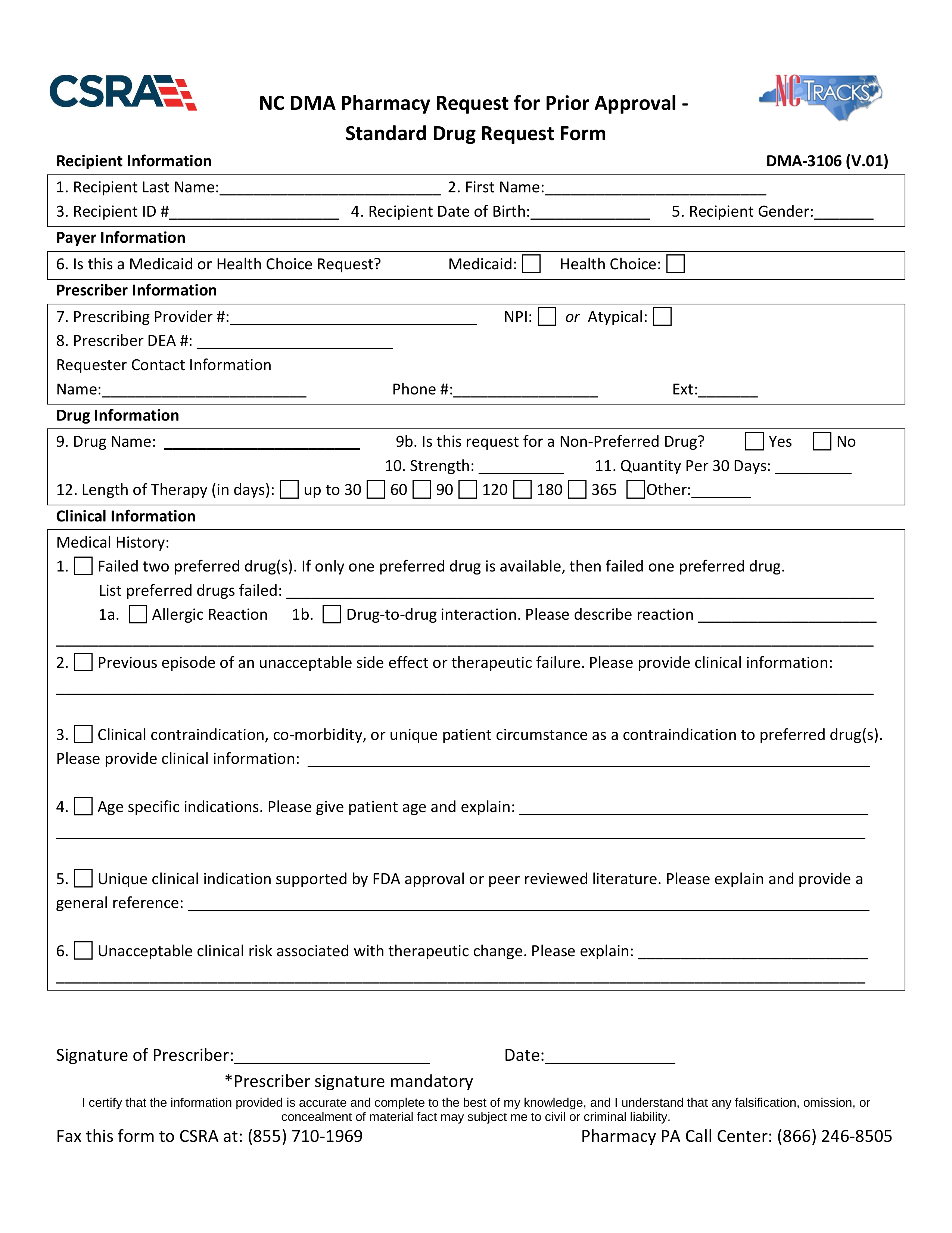
A North Carolina Medicaid prior authorization form is a document used by North Carolina-based medical professionals to request Medicaid coverage for a non-preferred drug. On the form, the person making the request must provide the medical justification for not prescribing a drug from the Preferred Drug List. The PA Call Center can provide more information about specific situations at the phone number provided below.
Fax – 1 (855) 710-1969
Phone – 1 (866) 246-8505