Signing Requirements
A principal must sign an advance directive in the presence of either two witnesses or a notary public.[1] Both witnesses must be competent adults, and at least one must not be related to the principal or stand to receive any portion of the principal’s estate.[2]
Registration
There is no requirement that an Arkansas advance directive be registered. It is recommended that the principal provide copies to their physician and to their designated health care agent.[3]
State Definition
“Advance directive” means an individual instruction or a written statement that anticipates and directs the provision of health care for an individual, including without limitation a living will or a durable power of attorney for health care.[5]
Statutory Form
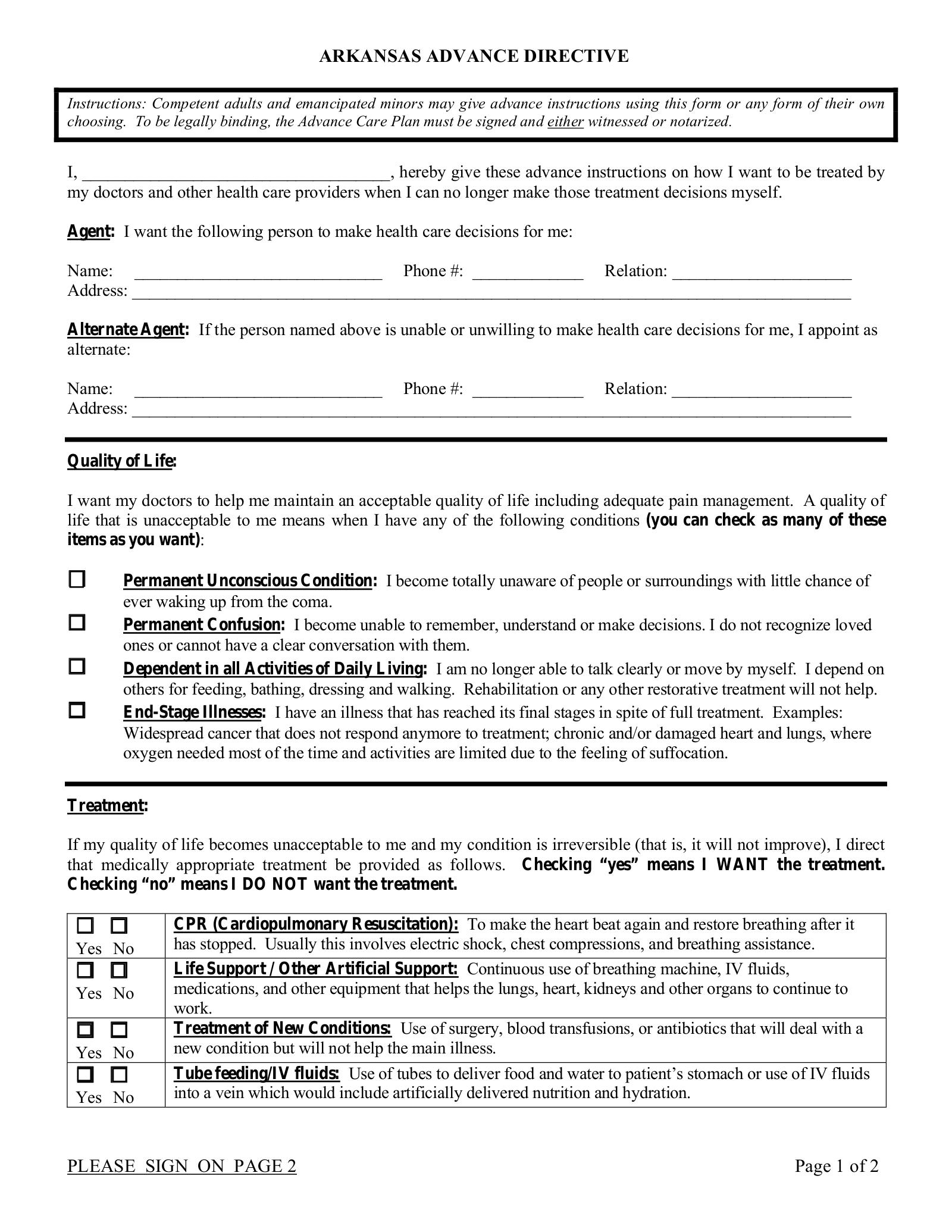
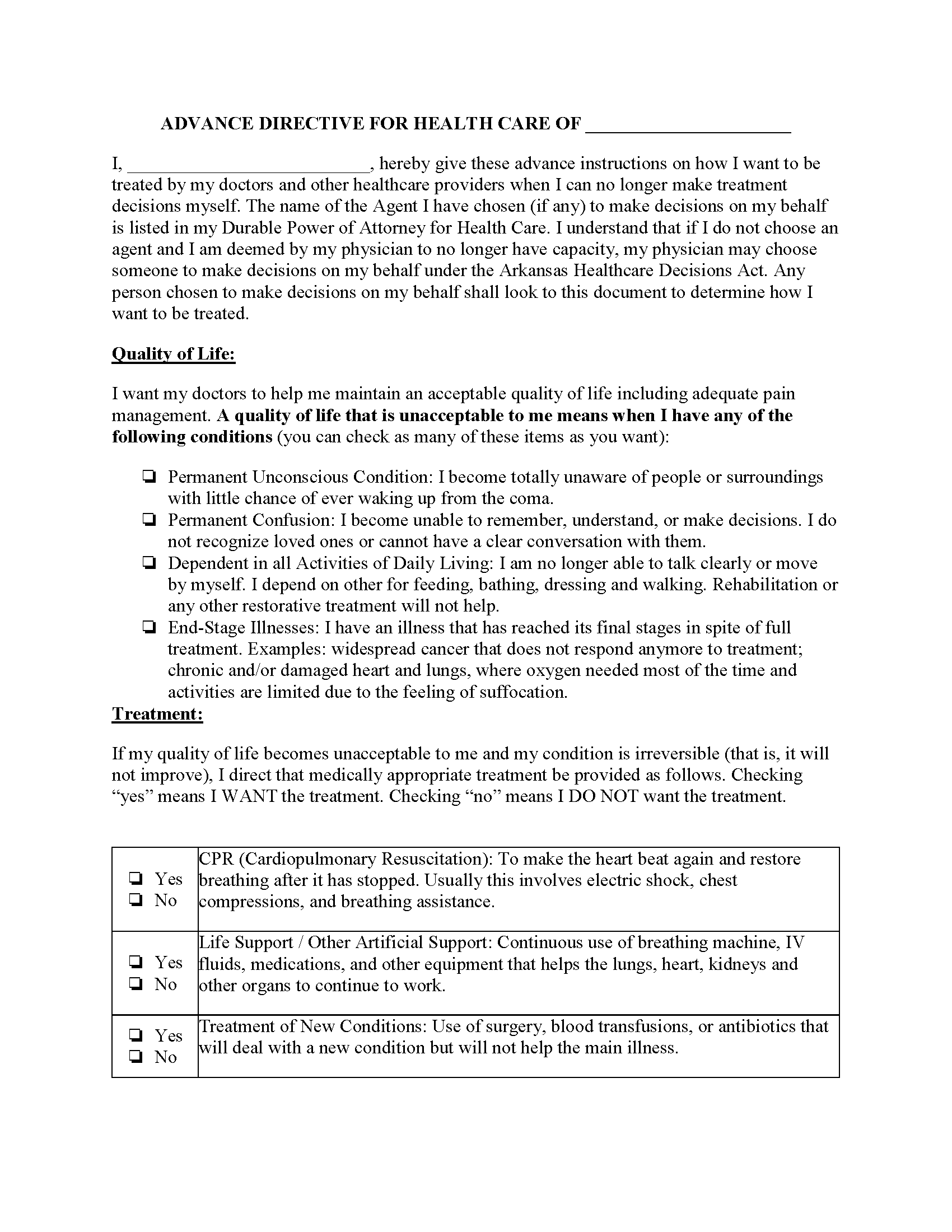
There is no statutory form. However, an Advance Care Plan form is available from the Arkansas Department of Health.
Sample
Download: PDF