Updated June 02, 2022
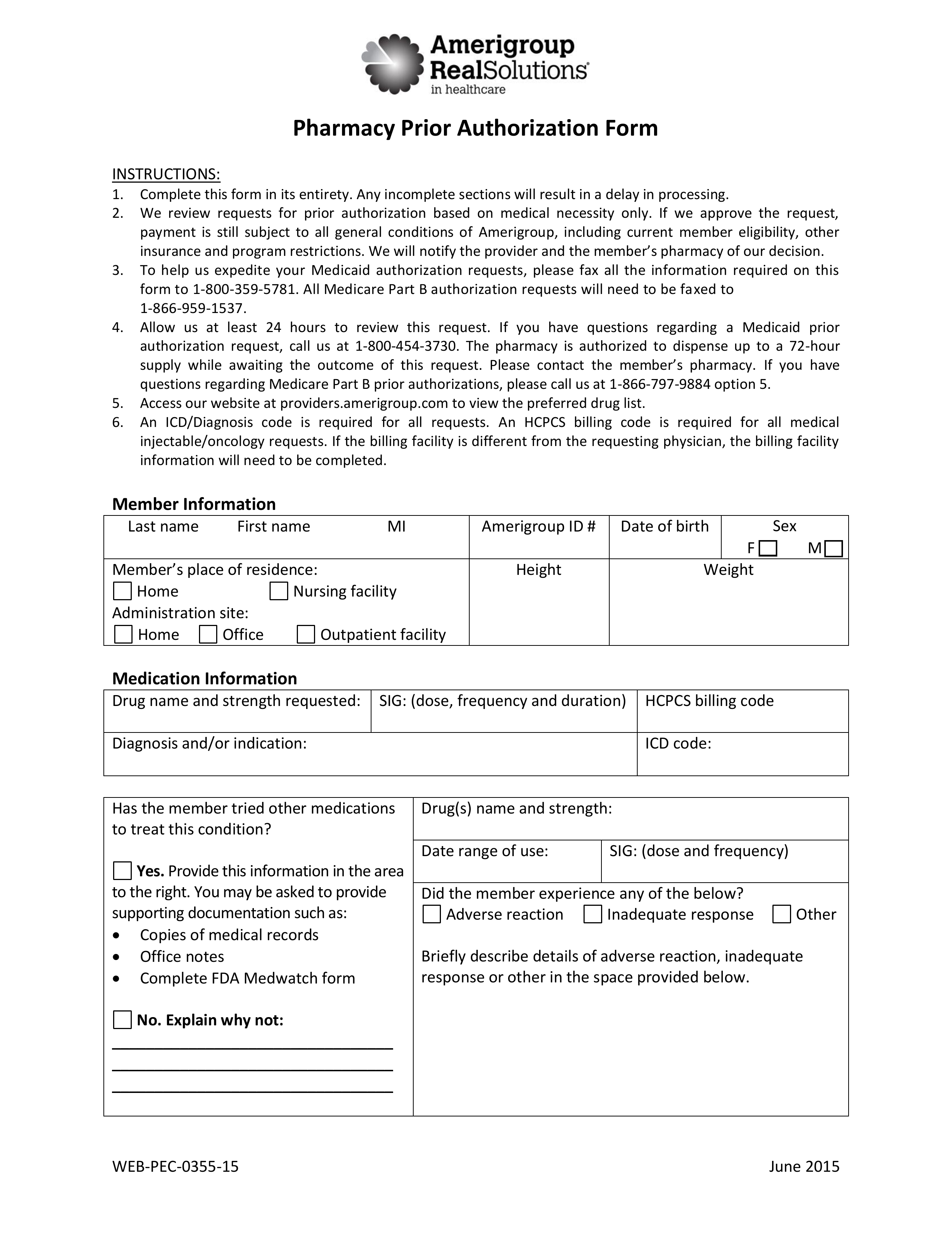
An Amerigroup prior authorization form is the document that should be used by patients insured by Amerigroup in order to receive approval for the cost of pharmaceutical treatment. A medical office requesting coverage for a patient’s prescription cost will often need to submit to the patient’s health insurance provider a prior authorization form. The form must be completed in its entirety before being faxed to the appropriate address below.
- Medicaid Fax: 1 (800) 359-5781
- Medicare Part B Fax: 1 (866) 959-1537
- Phone: 1 (866) 797-9884 option 5
How to Write
Step 1 – In “Member Information”, provide the member’s full name, ID number, date of birth, sex (m/f), place of residence, administration site, height, and weight.
Step 2 – In “Medication Information”, specify the drug name, strength requested, SIG, HCPCS billing code, diagnosis and/or indication, and ICD code.
Step 3 – Continue by specifying whether or not the patient has tried other medications to treat their condition.
- If yes, specify the drug name and strength, date range of use, and SIG. Also explain any adverse reactions, inadequate responses, or other details in that regard
- If no, explain why not
Step 4 – At the top of page 2, explain any medical necessities for non-preferred medication(s) or for prescribing outside of FDA labeling. Also, list all other medications (including dose and frequency) and explain any other pertinent information.
Step 5 – In “Diagnostic Studies and/or Laboratory Tests Performed”, list all tests done within the past thirty (30) days. For lab tests, explain the test, date, and result. For diagnostic tests, explain the procedure, test, and result.
Step 6 – In “Prescriber Information”, provide the prescriber’s full name, NPI number, and DEA/licence number. You must also supply the full address where services were rendered along with corresponding phone number, fax number, office contact name and their direct phone number.
Step 7 – In “Billing Facility Information”, supply the billing facility’s name, NPI/Tax ID number, DEA/licence number, full address, phone number, fax number, and the name of an office contact.
Step 8 – In “Pharmacy Information”, supply the name of the pharmacy, pharmacy NPI number, telephone number, and fax number.
Step 9 – The prescriber must provide their signature at the bottom of the page and date the signing.