Updated July 05, 2023
A West Virginia advance directive is a form that combines several health planning documents to allow a person to outline their end-of-life medical treatment preferences. The form also allows a person to select someone else, an “agent”, to act in their place and make medical decisions if the patient cannot do so for themselves. The agent must make decisions in accordance with the medical requests written in the advance directive.
Advance Directive Includes
Table of Contents |
Laws
Statute – Chapter 16, Article 30 (West Virginia Health Care Decisions Act)[1]
Signing Requirements – Two witnesses and a notary public.[2]
Versions (4)

Download: PDF
Download: PDF
Download: PDF
 Mental Health Advance Directive
Mental Health Advance Directive
Download: PDF
How to Write
Download: PDF
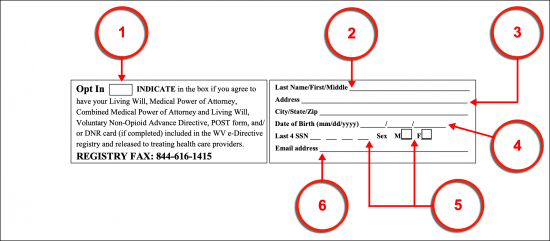
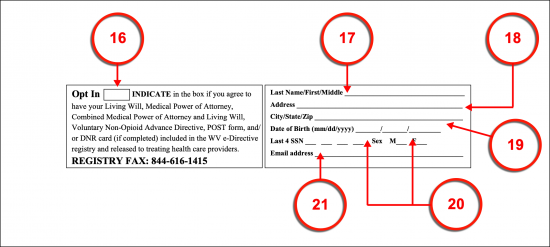
(1) WV E-Directive Registry Status. The West Virginia E-Directive Registry will store your medical directives and make them available to West Virginia Medical Personnel seeking your treatment preferences when you are unable to communicate or maintain consciousness. In order for this release of information to occur, you must provide approval. To approve of the West Virginia E-Directive Registry release of your medical directives to Health Care Providers, mark the box labeled “Opt In.”
(2) West Virginia Principal Name. Produce your full name as the West Virginia Patient who shall use this directive to convey treatment instructions to Medical Providers in this state.
(3) Address Of West Virginia Principal. Document your entire residential address utilizing the two areas provided.
(4) Principal Date Of Birth. Continue identifying yourself as the West Virginia Patient by reporting your date of birth.
(5) West Virginia Principal Information. The last four digits of your social security number should be documented along with a selection of either the “M” checkbox (male) or “F” checkbox (female) to indicate your sex.
(6) Email Address. Furnish your e-mail address to this header.
Medical Power Of Attorney
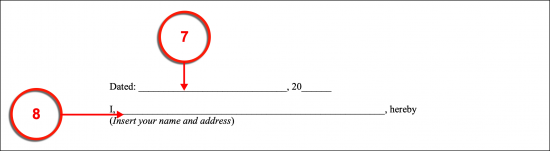
(7) Dated. Future West Virginia Medical Providers will wish to use the most recent appointment you have when you are incapacitated and unable to issue your own medical instructions. Therefore, produce the calendar date marking when you formally make this appointment at the beginning of this form.
(8) West Virginia Principal Name And Address. The full name of the West Virginia Principal along with his or her address must be inserted to this document’s declaration. Thus, furnish your name and address to this statement as the West Virginia Patient or Principal. It will be assumed that this document is being prepared by the West Virginia Patient it discusses.
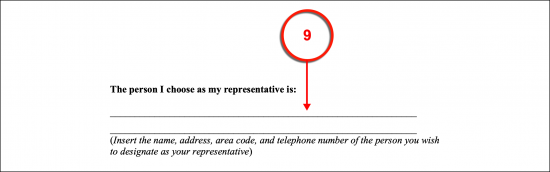
(9) West Virginia Health Care Representative Name And Address. Your choice of Health Care Representative should be displayed as well. This will be the only way future West Virginia Physicians will have of confirming that the Party you wish to represent your treatment preferences possesses your authorization to do so. Produce his or her entire name and current residential address. Note this Party may not be affiliated with any West Virginia Health Care Provider responsible for your medical treatment but may be a Relative or close Friend of your choosing.
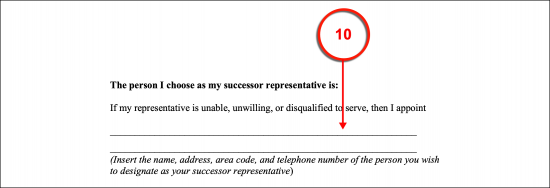
(10) West Virginia Successor Representative Information. In addition to the West Virginia Health Care Representative Appointment, the opportunity to name a West Virginia Successor Health Care Representative has been included with this appointment. This is a recommended option since there is the possibility that your initial appointment (made above) may not be able to fulfill this role at the time when West Virginia Medical Providers contact him or her. The Successor will not have any true principal powers while the original West Virginia Health Care Representative is in place. However, should the original choice be revoked, be incapacitated, unavailable, unreachable, or simply refuses for personal reasons then the exact same authority over your treatment decisions given to the West Virginia Health Care Representative will transfer immediately to the Successor you name. Dispense the Successor Representative’s full name as well as the residential address and phone number where he or she can be reached to the appropriate statement to fulfill this designation’s requirement.
(11) Confirm First Page. Regardless of whether you are filling this form out to define your medical directives (as the Patient) or whether you are a Preparer furnishing information at the request of the Patient, this page needs to be confirmed. To this end, the full name of the West Virginia Patient must be furnished at the bottom.
(12) Special Directives Or Limitations. Naturally, the West Virginia Health Care Representative and the Successor Representative will be trusted individuals whom you believe can reliably carry out the instructions you have issued to be followed when you are incapacitated, require significant medical attention, and must produce authorizations for treatment, but are unable to communicate or are unconscious. The West Virginia Health Care Representative will thus be given quite a scope of powers. For instance, he or she can approve or refuse surgeries for your treatment, authorize, or deny the application of tubes that will deliver nutrition and fluids when you are incapable of eating and drinking, handle your admittance to Medical Facilities, and even deny privately requested autopsies (he or she may not deny an autopsy that is required by Law Enforcement or similar institution seeking evidence of foul play). Some of these decisions can make the difference of life or death and this may prove to be difficult even for the most reliable of Parties. You may limit your Representative’s decision-making powers, dispense specific instructions to West Virginia Medical Providers and Health Care Representative, and even produce information and conditions to be applied for medications and procedures used for medical or mental health interventions.
(13) Principal Signature And Document Date. The West Virginia Patient must sign this document once sure that it accurately defines the appointment of treatment decision-making powers being granted to his or her Health Care Representative. Once this signature is complete, he or she is required to report the current date.

(14) Witness Signatures And Dates. Two completely impartial adults are required for the role of Witness. Each must attest to his or her status of not having any interest in the Principal’s health or assets, are adults, are not related at all to the Principal, not his or her Physician, Health Care Representative (or Successor Health Care Representative), and of observing your execution of this directive by signing the provided testimonial and dispensing the current calendar date.
(15) Notary Public Requirement. After the Witnesses have provided testimony the Notary Public overseeing the execution of the West Virginia Principal’s signing will complete the notarization process. He or she will provide proof of the completed process directly to this paperwork in the section provided.
(16) Living Will E-Directive Registry Status. The Living Will portion of this document can also be registered with the West Virginia E-Directive. It is imperative that your initials be supplied to the “Opt In” checkbox if you intend to register your medical preferences. This act will provide approval for West Virginia to make your directive accessible to attending Medical Personnel.
(17) Full West Virginia Declarant Name. The Patient issuing his or her treatment declarations for Medical Providers in the State of West Virginia should be identified with his or her name (presented as the last, first, then middle name). Claim this directive by entering your full name.
(18) West Virginia Declarant Address.
(19) Date Of Birth And Social Security Information. Record your date of birth as well as the last four digits of your social security number. These items will aid West Virginia Medical Professionals in solidifying your identity as the Patient behind this paperwork.
(20) Declarant Information. Indicate your sex by placing a mark on the “M” or “F” line.
(21) West Virginia Declarant’s Email Address.
Living Will
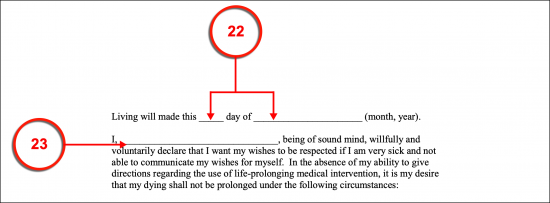
(22) Declaration Date. Present the official date of your declaration of treatment instructions when you are gravely ill, incapacitated, injured, or pronounced as being in a lifelong coma.
(23) West Virginia Declarant Name. Attach your name to the statement made. Here, you will inform West Virginia Medical Personnel that you both request and authorize the removal of all life-sustaining treatments when terminally ill/injured, fatally ill/injured, or in a lifelong vegetative state. If you are unable to communicate this wish at the time because you do not have the capacity to, this directive will convey this request (and authorization) to Physicians in this state. Review the statements made in this document carefully.
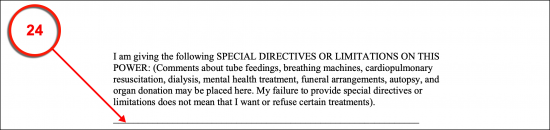
(24) Special Living Will Directives Or Limitations. This document will direct West Virginia Physicians to focus on comfort care over life-sustaining treatments in a basic manner that applies to nearly all situations. If you wish to provide additional statements such as requesting a trial period for invasive maneuvers like intubation, dialysis machine, and other technology that support organ function, or nourishment and water supplied through medical technology then, use the provided space to put your wishes in writing. You may cover any health care topics (such as the examples just given), mental health care treatments and interventions, hospice care, or post-death arrangements in this area as well. This can also be done on separate pages that are labeled properly and attached to this paperwork before it is signed.
(25) Principal Name. The full name of the West Virginia Principal should be produced in print to verify it is a part of this directive.

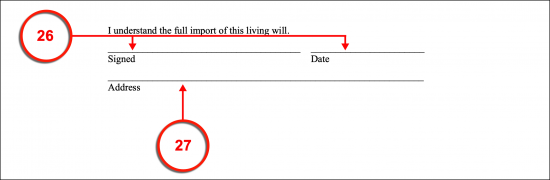
(26) Signed Name And Signature Date. Sign your name once you have gathered with two Witnesses and Notary Public then submit the current date.
(27) Address.
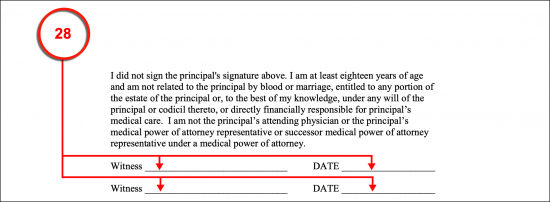
(28) West Virginia Witness Signature And Date. The two adult Witnesses present will both sign their names and provide their signature dates. It will be important that your signature date and that of these Parties are identical and define the current date when you sign this paperwork.
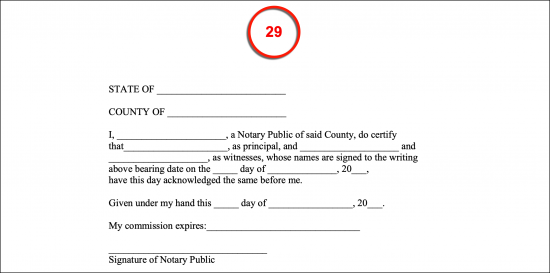
(29) Required Notarization. The Notary Public will now control this document. He or she shall complete the notarization section with the credentials needed to contact him or her in the future, the facts surrounding your signing, and the items needed to prove the notarization process is complete.
Release Of Information Authorization
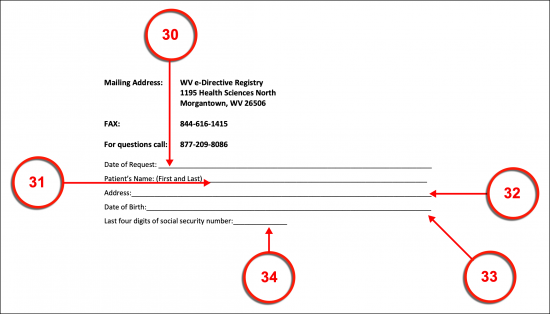
(30) Date Of Request. A basic form will need to be completed when a release of your directive is requested (by attending Physicians or you). It is generally a good idea to keep a copy of this form handy and to make sure your Health Care Representative has one. The first step in requesting a copy of your medical directives is a record of the date when the request is being made.
(31) Patient’s Name. Request the medical directives by naming the West Virginia Patient who issued them. Present this name in a standard first name/last name format.
(32) West Virginia Patient Residential Address.
(33) Date Of Birth. Disclose the birthday (month, calendar day, year) of the West Virginia Patient.
(34) Last Four Digits Of Social Security Number. The final four digits in the West Virginia Patient’s social security number will aid in confirming the paperwork requested belongs to the concerned Patient.
(35) Phone Number And Fax. The Requester’s telephone number and fax number should be presented.
(36) Recipient Request. Place a checkmark to indicate how this request can be sent. You may request that the West Virginia Patient’s directives be mailed to the Patient, sent to the fax number above, or both.
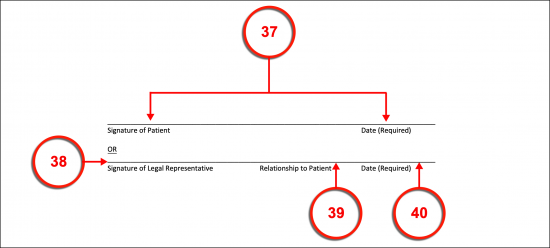
(37) Signature Of Patient And Date. The West Virginia Patient must sign this document in order to request a copy of his or her directives. This will also require that the current date be submitted.
(38) Signature Of Legal Representative. If the Legal Representative of the West Virginia Patient is seeking the concerned directive, then he or she should sign this area to affirm the request is genuine. In this case, the Patient is not obligated to sign this form unless the current directives make this a requirement.
(39) Relationship to Patient. The nature of the relationship the West Virginia Legal Representative has with the Patient should be defined.
(40) Signature Date.
E-Directive Registry Sign-Up Form
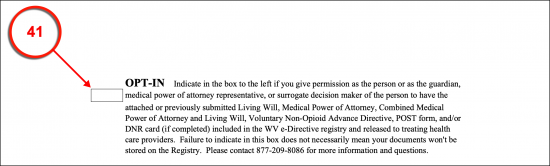
(41) Release Of Information Registry. The final form is an update to the registration process for the West Virginia E-Directive Registry and must be filled out for the registration process to be complete. You will also need to initial the “Opt In” box to give your Representative access to this form.
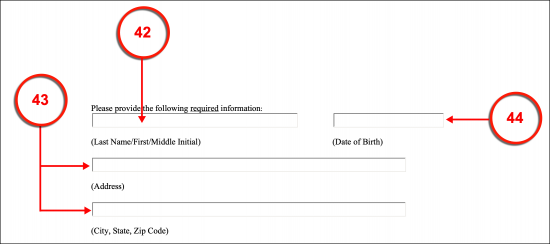
(42) West Virginia Declarant Name. The full name of the West Virginia Patient should be submitted along with his or her date of birth.
(43) Address Of West Virginia Declarant.
(44) West Virginia Declarant Date Of Birth.
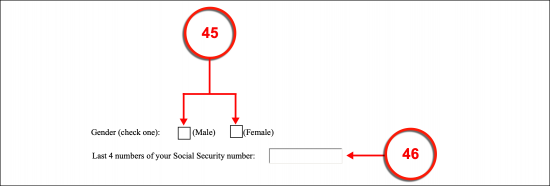
(45) West Virginia Patient Gender.
(47) Last 4 Numbers Of Social Security Number. The West Virginia Patient’s last four social security number digits should be displayed.
(47) Update As Purpose. If you have already completed the registration process but have moved and must update your address, then initial the “Demographic Updates…” box.
Related Forms
 Durable (Financial) Power of Attorney
Durable (Financial) Power of Attorney
Download: PDF, MS Word, OpenDocument

Download: PDF, MS Word, OpenDocument