How to Write
Step 1 – Download the dental insurance verification form in PDF.
Step 2 – In “Patient Information,” enter the patient’s name, SSN, and birthdate. Next, describe the patient’s relationship to the subscriber (insured individual).

Step 3 – In “Subscriber Information,” provide the subscriber’s name, SSN, birthdate, and subscriber ID #.

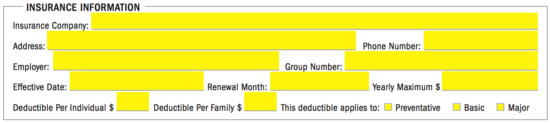
Step 4 – In “Insurance Information,” specify the following details pertaining to the subscriber’s insurance policy:
- Insurance company name
- Insurance company address
- Insurance company phone #
- Subscriber’s employer
- Group #
- Effective date
- Renewal month
- Yearly maximum ($)
- Deductible per individual ($)
- Deductible per family ($)
- Treatment(s) applicable to deductible
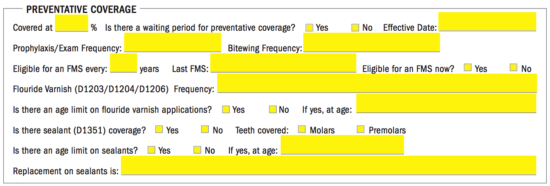
Step 5 – In “Preventative Coverage,” enter the following information related to the subscriber’s preventative coverage:
- Percentage of coverage
- Is there a waiting period for the preventative coverage?
- Effective date
- Prophylaxis/Exam frequency
- Bitewing frequency
- Fluoride varnish frequency
- Is there an age limit on fluoride varnish applications?
- If yes, at what age?
- Is there sealant coverage?
- Which teeth are covered? (molars, premolars)
- Is there an age limit on sealants?
- If yes, at what age?
- Replacement on sealants (describe)
Step 6 – In “Basic Coverage,” enter the percent which is covered for basic dental work and select “Yes” or “No” to specify whether there is a waiting period for basic coverage. Following that, specify the effective date of basic coverage and describe what the coverage includes.

Step 7 – In “Major Coverage,” specify the percent that the insurance plan will cover for any major dental work. Next, indicate whether or not there is a waiting period for major coverage and enter the effective date of said coverage. Lastly, mention what type of dental work the major coverage includes.

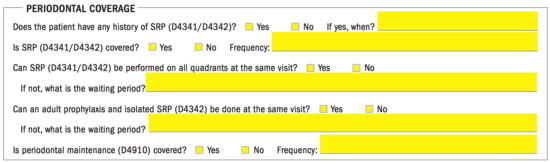
Step 8 – In “Periodontal Coverage,” the following details must be specified:
- Does the patient have any history of SRP (D4341/D4342)?
- If yes, when?
- Is SRP (D4341/D4342) covered?
- Frequency of SRP (D4341/D4342) coverage
- Can SRP (D4341/D4342) be performed on all quadrants at the same visit?
- If not, what is the waiting period?
- Can an adult prophylaxis and isolates SRP (D4342) be done at the same visit?
- If not, what is the waiting period?
- Is periodontal maintenance (D4910) covered?
- Frequency of periodontal maintenance (D4910)
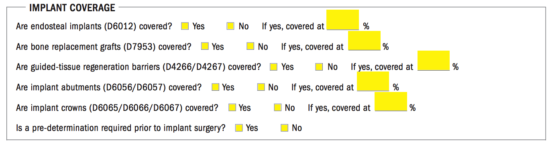
Step 9 – In “Implant Coverage,” respond to the questions by selecting “Yes” or “No”. Additionally, provide the coverage percentages for the corresponding questions (where applicable). The questions are as follows:
- Are endosteal implants (D6012) covered?
- Are bone replacement grafts (D7953) covered?
- Are guided-tissue regeneration barriers (D4266/D4267) covered?
- Are implant abutments (D6056/D6057) covered?
- Are implant crowns (D6065/D6066/D6067) covered?
- Is a pre-determination required prior to implant surgery?
Step 10 – In “Orthodontic Coverage,” specify whether or not orthodontics are covered by the insurance plan. If orthodontics are covered, enter the percent that is covered. Next, indicate whether or not there is an age limit for orthodontic coverage (if an age limit, specify the age). Finally, specify whether or not there is a lifetime maximum and, if there is, enter the lifetime maximum.

Step 11 – In “Miscellaneous,” provide the following information in the available fields:
- Are nightguards (D9940) covered?
- If yes, what percentage?
- Is nitrous oxide (D9230) covered?
- If yes, what percentage?
- Years before replacements on crowns and bridges
- Years before replacements on partial dentures
- Are prior extractions covered (missing tooth clause)?
Step 12 – In “Additional Notes,” enter any details which may assist the medical facility in their handling the claim.
Step 13 – Lastly, enter the name of the individual who completed the form and provide the date.
![]()