How to Write
Step 1 – Start by downloading the form in PDF format.
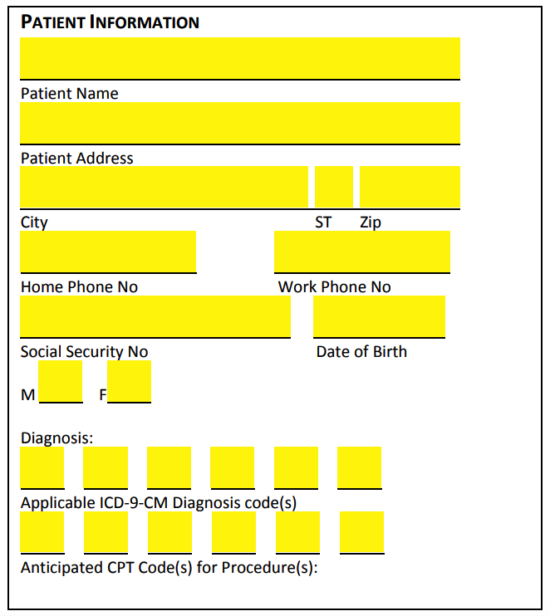
Step 2 – In the “Patient Information” portion of the form, specify the patient’s personal information by entering the following:
- Name
- Address (street)
- City
- State
- Zip
- Home phone #
- Work phone #
- SSN
- Date of birth
- Sex (M/F)
- Applicable ICD-9-CM diagnosis code(s)
- Anticipated CPT code(s) for procedure(s)
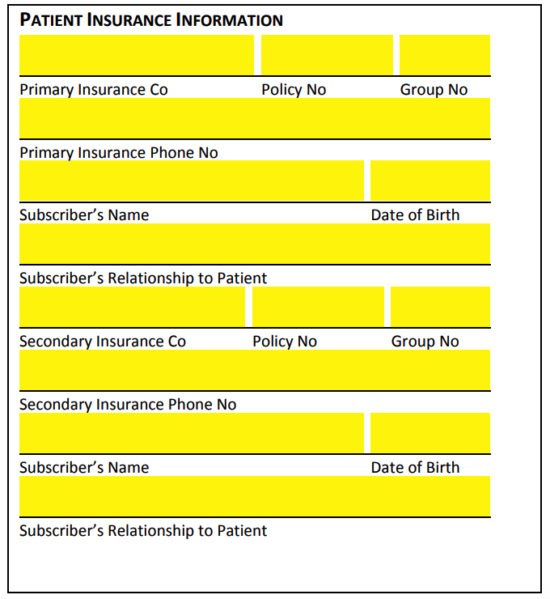
Step 3 – Next, in the “Patient Insurance Information” window, describe the patient’s insurance details by specifying the following
- Primary insurance company name
- Primary insurance company policy #
- Primary insurance company group #
- Primary insurance company phone #
- Subscriber’s name
- Subscriber’s date of birth
- Subscriber’s relationship to patient
- Secondary insurance company name
- Secondary insurance company policy #
- Secondary insurance company group #
- Secondary insurance company phone #
- Subscriber’s name
- Subscriber’s date of birth
- Subscriber’s relationship to patient
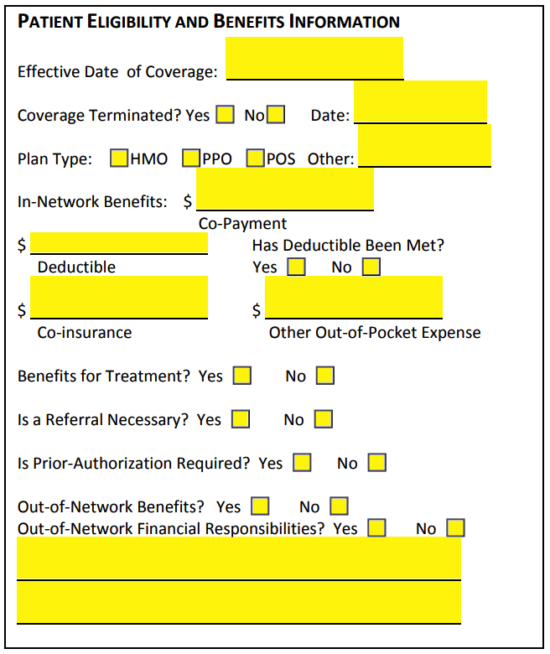
Step 4 – Continue on to “Patient Eligibility and Benefits Information” and specify the following details in the spaces provided:
- Effective date of coverage
- Coverage terminated?
- If yes, what date?
- Plan type (HMO, PPO, POS, other)
- In-network benefits (co-payment amount)
- Deductible amount
- Has deductible been met?
- Co-insurance amount
- Other out-of-pocket expense
- Benefits for treatment?
- Is a referral necessary?
- Is prior-authorization necessary?
- Out-of-network benefits?
- Out-of-network financial responsibilities?
- Additional information
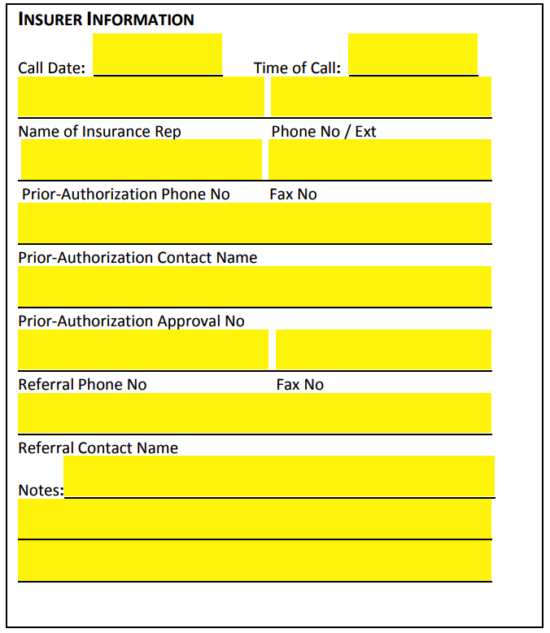
Step 5 – Lastly, in “Insurer Information,” describe the insurer’s details by supplying the following:
- Call date
- Time of call
- Name of insurance representative
- Phone # of insurer
- Prior-authorization phone #
- Prior-authorization fax #
- Prior-authorization contact name
- Prior-authorization approval #
- Referral phone #
- Referral fax #
- Referral contact name
- Additional notes